
PLANNING ON GETTING AN MRI? HERE'S WHAT YOU NEED TO KNOW FIRST.
Jun 28, 2022So first , let me start off with if your provider (or you) have legit reasons to think cancerous tumors are present, then absolutely, get that image!! Same goes for a trauma like a major car accident or falling off a high surface - there are certain times where imaging is warranted and necessary to make sure something truly major isn’t going on.
Outside of that, chances are this can save you LOTS of money and time (because imaging isn’t cheap and often can take awhile to get authorized/scheduled)…
Let me start by saying pain is super complex. There are a number of tissues in the body that can get irritated or inflamed and set up an alarm signal in your brain that then translates to pain in a region. And that pain may actually not even show up in the same area as where the signal originated from. There are all sorts of referral patterns or crazy ways that pain show up. Hell, just last week I saw someone with wrist pain that was coming from the shoulder and another with knee pain that was coming from the low back, and another with a headache coming from the neck. Past that, there’s also so many other psychosocial and environmental factors that go into pain - How are you sleeping? What’s your diet like? Are you managing stress effectively? Even FEAR of pain can even cause physical pain! The very act of thinking “I can’t deadlift anymore because I have degenerative disc disease and it is always going to hurt” can actually bring on pain before you even perform the lift! So while MRIs and other diagnostic imaging has it’s place, it’s often unnecessary and not really giving us any legit information about where your pain is coming from anyways. When it comes to musculoskeletal pain, the vast majority of the time we can get better and more accurate info on what’s going on and how to best treat it through a thorough history and physical examination versus any image.
Let’s go through a few studies that drive this home…
I wanna start with this big study on low back findings because one of the more common things I hear is “oh, I had a disc bulge years ago, so I can’t do XYZ and it’s why I have so much pain.” Honestly, someone (or society) along the way did you a disservice by leading you to believe that. And then our beliefs and expectations drive our outcomes, so it’s no wonder you’re still dealing with pain. I’m not saying it’s in your head, but at the same time…it is your brain that’s allowing the pain to continue at that point.
Did you know that EVERY clinical guidelines for physicians for the treatment of nonspecific low back pain (LBP) IN THE WORLD explicitly says that imaging is NOT recommended and SHOULD NOT be done unless there’s cause to believe a space-occupying-lesion (MRI or CT scan) or major fracture (xray) may be present?!?! Now as to why physicians aren’t following their own clinical guidelines….it’s either because they haven’t kept up with the research and seen their own updated guidelines OR it’s because insurance companies still reimburse for these at high rates.
There are several reasons why imaging isn’t recommended/warranted except in the case of major red flags. The biggest one is because at this point, research has solidly proven that no matter what tissue damage we find on imaging, we CANNOT correlate it to that persons symptoms. One of the research studies that determined this is one done by Brinjikji, wt al in 2014 where they took hundreds of people in all decades of life with NO PAIN and had them get imaging. So what did they find?! All kinds of things!!!! I’ll post the graph of the results below, but the gist is that it would highly abnormal for your image to show nothing regardless of what symptoms you may or may not be having. And if all of the people in this study can have all kinds of “terrible” findings on their image, yet have no pain, why can’t anyone else also not have any pain?! The answer is they can. You can have multiple disc bulges, labral tears, etc and have absolutely NO PAIN and function just fine. Hell, think of these things as normal signs of aging, kind of like wrinkles.
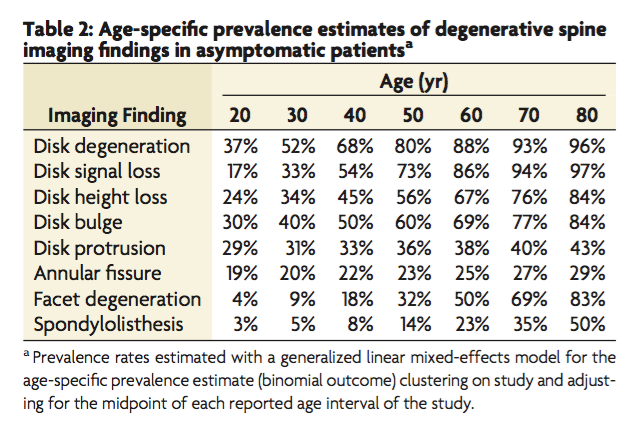
(asymptomatic = ZERO symptoms/pain/functional limitation)
Another study on “abnormal” knee findings using MRI in asymptomatic patients in their 50’s to 70’s found similar findings. The list of things they found include damage to the cartilage lining of the femur, underlying bone damage, meniscus injury, and more. Yet these were again all people with NO pain or dysfunction. And as before, the prevalence of the findings increased with age in the study participants. This once again demonstrates that there appears to be a normal amount of wear that occurs to the knees over a lifetime, yet it doesn’t necessarily correlate with the patient experiencing pain.
What about the shoulder? Minagawa et al did a study where they did imaging on both shoulders of 664 participants and found full thickness rotator cuff tears in 147 of those people. But how many were experiencing symptoms? Only 34.7%. The other 65.3% had zero symptoms! So again, a solid number of the ones experiencing pain could go through conservative care to get out of pain and get stronger.
Here’s a photo that shows a good overview of what “abnormal” findings may actually be normal or at least can be treated conservatively to get you out of pain and back to doing all the things:

And if these studies doesn’t convince you, I’ve got personal experience. I still have multiple disc bulges throughout my neck and back as well as some tearing in my rotator cuff and right labrum - possibly the left, too, but it’s never been imaged - and I still do all the things in CrossFit, weightlifting, and outdoor sports. And the only reason I ever got those images to know those results is because of major traumatic falls and car accidents that warranted imaging to check for fractures, etc, or they were back when I still had corporate health insurance and it required an image (a rant for another time). But I’d assume all of those things had already been there (except for the labrum which showed up after a really bad snowboarding fall - and yes, I treated that without surgery) and there is absolutely no way to know when they showed up. Hell, the disc bulges in my neck were found after 2 separate car accidents years apart with zero change in how they showed up on image…yet I had neck pain the first time I got the imaging (from something else entirely, though that didn’t stop medical providers from trying to blame them *eye roll*) and ZERO pain the second time. Hmmm….doesn’t sound like those had anything to do with my pain, right? If any provider ever tells you something like “oh this disc bulge here is from X incident…” Unless you legit had imaging the week prior to X and it wasn’t there, they are making an assumption at best. And even so, you cannot create a causative link between any musculoskeletal image finding and a person’s pain like we saw in that study above. For that matter, if you ever have a provider say that any specific musculoskeletal tissue is the cause of your pain, they are lying. Now don’t mishear me - I bet they mean well. And it might be a very educated guess they are making, but it’s just that - a guess. There is no way for us to know if any specific tissue is “at fault”…but what we CAN say based on our assessment is what general area is causing the pain and based on how an individual is presenting, we can come up with a really solid plan of care to get them out of pain and back to doing everything they need/want to.
Here’s another fun thing to consider:
If you don’t like your image results, go down the road and get another! It’ll likely be different!
Yes, I am aware of how grossly a generalized statement that is, but research has proven to show that results can and will be biased by whoever is reading it. Herzog at al is a research study where they took one 63 year old woman with LBP, including radicular symptoms (meaning she had symptoms down one leg) and had her get imaging at 10 different MRI centers within a 3 week period and looked at whether or not the reports were similar between the 10. Findings: little to NO consistency between them!!! In fact, there were 49 distinct findings across the 10 reports and about 33% of those findings were only in 1/10. I don’t wanna bog y’all down with the research (though feel free to email me with any questions if you do want to discuss it!), but yea, basically your imaging legit isn’t telling me much.
This variability is concerning since a lot of times our imaging is what’s referenced as to why a treatment is done or what’s covered by insurance, etc. But I think the big takeaway is to stop putting so much stock in an image especially when it comes to musculoskeletal pain. Again, tumors and such are a vastly different story here, but if we know that things like disc bulges or rotator cuff tears are relatively “normal” and are in plenty of people without any pain…AND we know that the results on our image reports differ based on who’s reading them…then what’s the point?? Honestly, I think there isn’t one. And most of the time, the “findings” on it are relatively normal. Hell, if you’re over the age of 20, I can pretty much guarantee that there will be “aBnOrMaL findings” found that are actually completely normal and don’t mean anything about your symptoms. The only times I suggest people get one is if there are major red flags present (things that point towards tumors or spinal cord issues or a traumatic event where the patient fits the criteria for imaging first) OR if we’ve really tried everything that should work for awhile without the expected results.
Ok, I’m gonna stop rambling and spouting research now. I think you get the point - you probably don’t need that image. And if a provider says you do, ask why. Use this blog and it’s info as a resource to advocate for yourself against unnecessary imaging and medical charges. And I would absolutely LOVE to discuss this further with anyone, so please - I’m looking forward to any and all questions.
Much love y’all,
Megan
P.S. Did you know that you could use membership sessions with me to really discuss any musculoskeletal thing you have questions about?! Think of it like consulting Google expect you get personalized results and advice that aren’t given based on SEO or ad costs. I already have a few people that we started out addressing a specific injury concern or made sure they could get back into X activity without issue and then transitioned into a mix of addressing anything that came up in the last month and then coaching/consulting on things like this! Check out memberships here
SUBSCRIBE FOR WEEKLY LIFE LESSONS
Lorem ipsum dolor sit amet, metus at rhoncus dapibus, habitasse vitae cubilia odio sed.
We hate SPAM. We will never sell your information, for any reason.
